
Climate disasters and mental health
by Robin Cooper, MD and Lise Van Susteren, MD
June 1, 2023
Share this entry:
What are climate disasters?
Climate disaster is a general term commonly used to describe catastrophic consequences of human-caused climate change.
While climate disasters include the impacts from slower moving chronic conditions, such as sea level rise, melting permafrost, and extinction of species, the focus in this entry will be on acute events. Acute events include extreme weather events (EWEs): fires, floods, storms (hurricanes and tornados), and heat waves. While no individual EWE can be attributed to the climate crisis, the global increase in temperature from greenhouse gas emissions has increased the frequency and intensity of EWE.s
EWEs and chronic climate disasters directly and indirectly strain our economies, our politics, and societies in general. The direct, ripple effects, and cumulative toll of this strain affects our personal mental health, that of our families, and collectively, our communities. It can define and destabilize nations – and ultimately our world.
Climate-driven disasters have increased by factor of five in the last half century (from 1970–2019), according to the World Meteorologic Organization. The United Nations Office for Disaster Risk Reduction reported that in the two decades from 1995–2015 alone, worldwide disasters have wounded, displaced, or required emergency assistance for four billion people; half a million people have died.
What is disaster mental health?
Disaster mental health focuses on the emotional toll of climate disasters and the urgent need to integrate psychological care into all disaster response programs. Psychological care includes mental health evaluation first aid, treatment, and consultation in the context of disasters.
How do climate disasters impact mental health?
Emotions: Although studies quantifying emotions associated with disasters are limited, ordinary human empathy can tell us a lot: When the place you call home is burned down by wildfires, blown away by tornados, flooded or leveled by hurricanes; when you lose your possessions, maybe your pets, your livelihood, the comfort and predictability of everyday life in a familiar community; witness injuries, illnesses, and deaths – the resulting mix of fear, anger, sorrow, and trauma can easily send a person into overwhelming states of distress.
The graphic below shows the common emotional and behavioral responses to disasters. (Reproduced with permission from Morganstein and Ursano, 2020.)

- Distress reactions: In the face of trauma from disasters, people can experience a range of distress reactions, from feeling dazed and in temporary shock, to a destabilizing sense of deep vulnerability. These are normal reactions.
- Health risk behaviors: In an attempt to cope, people may engage in problematic behaviors, adding to the existing challenges faced from the disaster.
- Psychiatric disorders: Research shows that stress from climate disasters can lead to new psychiatric disorders or exacerbate pre-existing conditions, such as major depression, anxiety, PTSD, adjustment disorders, an increase in drug and alcohol abuse, and domestic violence – including child abuse. Not to be overlooked is the loss of place that erodes one’s identity and feeling of belonging – important components of mental well-being. These feelings can linger for months to years.
- Resilience: Although significant emotional and psychiatric difficulties are experienced, many people do recover with resolution of their distress. (See “Reconstruction Phase” below.)
Typical phases of disasters
Disaster mental health experts have identified common patterns of individual and community reactions to disasters. These are illustrated below. (Reproduced with permission from Morganstein and Ursano, 2020.)
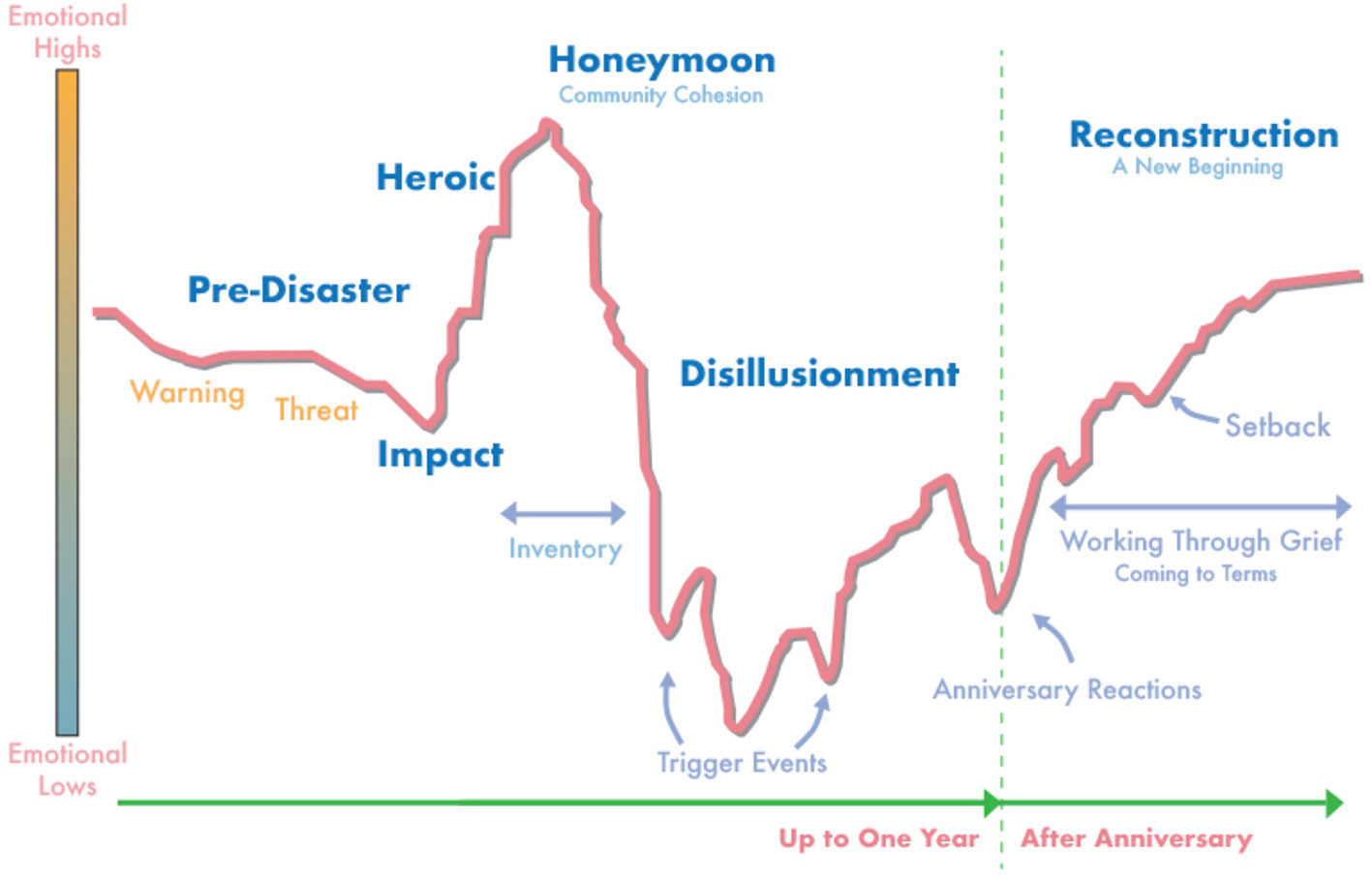
Pre-disaster Phase: Anticipatory fear is experienced in the early stages, followed by the trauma of the event itself. Timely warnings can give the opportunity to take safety measures, which can reduce the feeling of helplessness and boost the feeling of having (some) control. In contrast, denial of the danger leads to avoidance and inaction, heightened vulnerability to disaster, and a more pervasive sense of helplessness.
Impact Phase: After a natural disaster, an identifiable low point is seen, followed by the feeling that the worst is over, and the recovery process can begin.
Heroic and Honeymoon Phases: These occur in the immediate aftermath of a disaster. They are marked by shows of altruism, generosity, and a sense of shared purpose. Vows to rebuild, replant, and restore are often heard. As people reach out to assist each other, a sense of community cohesion is often felt. This phase often draws media attention showing scenes of heroes rescuing those in need. Such attention from the outside world helps people feel that the rest of the world “cares”.
Disillusionment: As time goes on, recovery may be prolonged; the response to the harms and destruction may be experienced as inadequate to the needs of the impacted people. Community cohesiveness may fade. Disillusionment and cynicism can replace the prior sense of hopefulness. A range of uncomfortable emotions may emerge: despair, anger, helplessness, sorrow and grief at the losses. Feelings of invisibility and abandonment may emerge, driving outrage directed at the government for not providing enough help, and for not taking enough preventive measures. Similar feelings may be directed at other entities. This phase can persist depending on the availability of resources and adaptive capacities.
Reconstruction Phase: This phase is defined by the period when an individual or community attempts to come to terms with the actual event, faces and grieves losses, and confronts the emotional aftermath of life after the trauma. This “new beginning” is a time when the focus is on moving forward. An anniversary of the disaster and other triggers, however, may cause symptoms and setbacks to this process.
How we “carry on” after a climate disaster is influenced by many factors, including our backgrounds, current mental states, life experiences, resources, personalities and temperaments. The nature of the event itself plays a role in influencing the extent of psychological injury: the intensity of the feeling of powerlessness generated, the “merciless” character of incidents, the pace, suddenness, degree of damage, loss of life and injury and the extent to which people personalize these incidents.
Beyond the phases: The upward trend in the image of the “Reconstruction Phase” implies the promise of improvement and resolution. However, recovery is far more complex, and far from guaranteed. While many victims of climate-related EWE may return to prior functioning and successfully rebuild their lives, those with the fewest resources and least support may not be able to put their lives back together and risk suffering enduring associated emotional sequelae.
What’s more, those who experience repeated or ongoing disasters may not have a chance to recover emotionally before the next disaster hits. This compounds the harm because each disaster deepens emotional vulnerability. Vulnerable communities may become defined by the impacts of repeated climate trauma.
Anxiety among those who fear that another climate disaster may be just around the corner can rise to the level of “pre-traumatic stress“. For example, residents of New Orleans have reported that just seeing a storm cloud can trigger anxiety of flooding.
Unequal impacts
The impacts of climate disasters are “brutally unequal“. Vulnerable and special groups particularly at-risk during climate disasters include:
- The elderly: Seniors may experience reduced mobility, hearing, and vision, and more medical conditions, which interfere with their ability to move quickly out of harm’s way. They may also have cognitive impairments, which compromise their ability to judge danger and their willingness be displaced. In the short-term, rescuing these individuals may be a challenge; in the long-term, they can require more care and help with daily living activities.
- Children: Because young people must count on the physical and mental competency of adults to survive and thrive, compromised care following a disaster can be profoundly harmful to children physically and emotionally. This will add to their existing stress from the disaster, and the consequences can reverberate throughout their lives. For some, the sense of security will be permanently altered. For a given traumatic event, studies show that children are especially vulnerable and are more frequently diagnosed with depression, sleep disorders, behavioral disorders and PTSD. Some may suffer from pre-traumatic stress as they envision future disasters.
- People with disabilities: People with disabilities are less equipped to grapple with an emergency brought on by an EWE; for example, people with mobility issues, or who are blind or hearing impaired, may be less able to quickly evacuate. They may face a steep(er) curve as they work to cope with unfamiliar surroundings and conditions post-disaster.
- People with pre-existing illnesses, including mental illness, substance abuse, and other medical conditions.
- Institutionalized individuals, including prisoners, nursing home residents, and rehabilitation residents.
- People experiencing homelessness or who live in substandard housing.
- Women, especially pregnant women and single mothers. Research shows that violence against women and girls can increase following natural disasters.
- Our “heroes”: First responders, including firefighters, police, emergency medical technicians, and other health and medical personnel. Two reviews (by researchers at the Center for the Study of Traumatic Stress and Aberdeen Centre for Trauma Research) have found that first responders experience higher rates of PTSD, depression, and anxiety.
Poverty and the biases linked to racism are “multipliers” of risk because they impede access to the resources that help individuals and communities endure, recover and adapt. At greatest risk are areas in developing countries, where poverty is widespread and resources are limited.
Consequences if we don’t reduce carbon emissions drastically
The intensity and frequency of hurricanes, floods, heat-related events, wildfires and other human-caused natural disasters will continue to increase.
Our mental health care system is already stretched to the limit. It is grossly unprepared to respond to the rapidly unspooling effects of the climate crisis. Calls for mental health professionals to help with the mounting psychosocial toll will become more intense; can we doubt that they will feel overwhelmed? Now is the time to shape an approach that prepares us for the responses that will be needed. The current model – a one-to-one delivery approach – is not sufficient, and will need to cede ground to a public health model, with an all hands on deck, community-wide and population-based approach. Collaboration with experts specifically trained for this new approach will be a critical component.
Addressing the impacts of climate disasters
It is essential that mental health care be integrated into the emergency trauma response to climate disasters.
While the Federal Emergency Management Agency (FEMA) and other entities such as the Red Cross respond to disasters, their work is primarily focused on physical impacts. Psychological care has not been adequately provided, despite overwhelming research documenting the psychological and behavioral health consequences.
Disaster response requires a multidisciplinary approach: People who have specialty training and experience as first responders, emergency medical technicians, and disaster management experts capable of coordinating services with different entities (multiple governmental agencies, physicians, and other health care providers). There is a significant gap in addressing the impact of disasters on mental health. So far, mental health professionals have played a limited role in disaster preparation and response. This gap cries out to be closed.
Mental health professionals have unique skills to bring to the needs of communities and individuals following disasters. Disaster response training for mental health professionals should be made available in the programs of all disciplines related to mental health. Training should include:
- Disaster preparation: Integration of mental health considerations and interventions into training multidisciplinary disaster response teams. Research shows that collaboration among public health stakeholders (for example, local health departments, academic health centres, and faith-based organizations) can plan and implement effective disaster mental health preparedness plans. Mental health professionals should be trained to work with disaster management experts, community organizations, governmental agencies, first responders, schools, and other entities to plan for coordinated responses.
- Disaster Response: providing on the ground “emergency” psychological first aid.
- Assistance in shaping public messaging.
- How to identify people most vulnerable to severe psychological responses to ensure no traumatized group is overlooked, and to prioritize resources for those most in need. This is a nuanced assessment that not only protects the vulnerable, but prevents over pathologizing or prematurely labeling those having acute stress reactions, which may not last long-term.
- How to identify and advocate for the establishment of safe spaces and practices conducive to recovery for the special needs of vulnerable populations.
- Teaching basic coping skills.
- Recovery interventions: Coordinating care and resource provision for affected individuals and groups alongside primary care providers, disaster agencies, and community organizations.
- Follow up: After early recovery efforts, ongoing support for the long-term needs of those with persistent difficulties must not be ignored.
What more might we need to know?
Action areas for research, policy, and practice include:
- Defining best practices for interventions that can be scaled up for large populations.
- Establishing metrics to measure progress.
- Designing treatments to address the impacts of multiple traumas from repetitive disasters.
- Persuading professional organizations to immediately begin the process of creating a skilled workforce trained to meet the growing psychosocial vulnerabilities.
- Creating a subspecialty in climate change and mental health to train mental health professionals is urgently called for.
We know a lot about what is needed to address climate change and develop energy sources that break our reliance on fossil fuels – the drivers of climate change and climate disasters. What we need to do now, more than anything, is to turn what we know into what we do.
What can I do if I need help after a climate disaster?
- Contact SAMHSA’s Disaster Distress Helpline at 1-800-985-5990, a 24/7, 365-day-a-year, national toll free, multi-language, confidential hotline with crisis counseling for people who are experiencing emotional distress related to any natural or human-caused disaster.
- Contact the National Crisis Lifeline via: Call 988, text 988, or chat at 988lifeline.org.
- Contact the Crisis Textline: Text TALK to 741741.
- Take a look at the Climate Resilience for Frontline Clinics, a collection of resources for U.S. health care providers, patients and administrators. Developed in collaboration with the Harvard T.H. Chan School of Public Health.
- The American Psychiatric Association offers an extensive list of resources for Coping After Disaster.
- Read over SAMHSA’s Coping Tips for Traumatic Events and Disasters, including a list of resources.
- SAMSHA offers a summary of stress management techniques for disaster responders, including a list of resources.
Further reading
Articles and Online Sources
Behavioral Health Conditions in Children and Youth Exposed to Natural Disasters, published in the Supplemental Research Bulletin in September 2018, by the Substance Abuse and Mental Health Services Administration (SAMHSA) Disaster Technical Assistance Center (DTAC).
Consensus Conference on the Role of Psychiatrists in Disaster, published by the Uniformed Services University of the Health Sciences (USUHS), Bethesda, Maryland in September, 1997, edited by Robert Ursano and Ann E. Norwood.
Disaster risk out of control despite global agreement to stop them, published by the United Nations Office for Disaster Risk Reduction on April 5, 2023.
How Climate Change Makes Child Abuse Worse, published in Moms Clean Air Force, on September 27, 2016, by Molly Rauch.
Mapped: How climate change affects extreme weather around the world, published in Carbon Brief on August 4, 2022.
New Orleans Scrambles to Repair Drainage System After Severe Flooding, published in The New York Times, on August 11, 2017, by Katy Reckdahl.
Our children face “pretraumatic stress” from worries about climate change, published in The BMJ Opinion on November 19, 2020, by Lise Van Susteren.
Protecting older adults from the effects of natural disasters and extreme weather, published by the National Institute on Aging on October 18, 2022.
Resource Document on Mental Health and Climate Change, published by the American Psychiatric Association in 2017, by Robert J. Ursano, Joshua C. Morganstein, and Robin Cooper.
The human cost of weather-related disasters 1995-2015, published in 2015, by the Centre for Research on the Epidemiology of Disasters and United Nations Office for Disaster Risk Reduction.
Weather-related disasters increase over past 50 years, causing more damage but fewer deaths, published by the World Meteorological Organization on August 31, 2021.
Organisations
American Psychiatric Association, Disaster Mental Health
American Psychological Association, Disasters and Response
Centers for Disease Control and Prevention, Emergency Preparedness and Response
Substance Abuse and Mental Health Services Administration (SAMHSA), Disaster Preparedness, Response, and Recovery
U.S. Department of Homeland Security, Ready
Selected Research/Scientific Papers
Alexander, D. A., & Klein, S. (2009). First responders after disasters: a review of stress reactions, at-risk, vulnerability, and resilience factors. Prehospital and disaster medicine, 24(2), 87–94. https://doi.org/10.1017/s1049023x00006610
Benedek, D. M., Fullerton, C., & Ursano, R. J. (2007). First responders: mental health consequences of natural and human-made disasters for public health and public safety workers. Annual review of public health, 28, 55–68. https://doi.org/10.1146/annurev.publhealth.28.021406.144037
Benevolenza, M.A., & DeRigne, L. (2018). The impact of climate change and natural disasters on vulnerable populations: A systematic review of literature. Journal of Human Behavior in the Social Environment, 29, 266 – 281. https://doi.org/10.1080/10911359.2018.1527739
Cooper, R., & Duncan, R. (2023). Special report: Wildland firefighters—hidden heroes of the mental health effects of climate change. Psychiatric News, 58(05). https://doi.org/10.1176/appi.pn.2023.05.5.38
Davidson, J. R., & McFarlane, A. C. (2006). The extent and impact of mental health problems after disaster. The Journal of clinical psychiatry, 67 Suppl 2, 9–14. PMID: 16602810
Fisher, S. (2010). Violence Against Women and Natural Disasters: Findings From Post-Tsunami Sri Lanka. Violence Against Women, 16(8), 902–918. https://doi.org/10.1177/1077801210377649
Giarratano, G., Harville, E. W., Barcelona de Mendoza, V., Savage, J., & Parent, C. M. (2015). Healthy start: description of a safety net for perinatal support during disaster recovery. Maternal and child health journal, 19(4), 819–827. https://doi.org/10.1007/s10995-014-1579-8
Goldmann, E., & Galea, S. (2014). Mental health consequences of disasters. Annual Review of Public Health, 35(1), 169–183. https://doi.org/10.1146/annurev-publhealth-032013-182435
Kousky, C. (2016). Impacts of natural disasters on children. The Future of Children, 26(1), 73–92. https://doi.org/10.1353/foc.2016.0004
McCabe, O. L., Perry, C., Azur, M., Taylor, H. G., Gwon, H., Mosley, A., Semon, N., & Links, J. M. (2013). Guided preparedness planning with lay communities: enhancing capacity of rural emergency response through a systems-based partnership. Prehospital and disaster medicine, 28(1), 8–15. https://doi.org/10.1017/S1049023X12001483
McCabe, O. L., Semon, N. L., Lating, J. M., Everly, G. S., Jr, Perry, C. J., Moore, S. S., Mosley, A. M., Thompson, C. B., & Links, J. M. (2014). An academic-government-faith partnership to build disaster mental health preparedness and community resilience. Public health reports (Washington, D.C. : 1974), 129 Suppl 4(Suppl 4), 96–106. https://doi.org/10.1177/00333549141296S413
Morganstein, J. C., & Ursano, R. J. (2020). Ecological Disasters and Mental Health: Causes, Consequences, and Interventions. Frontiers in psychiatry, 11, 1. https://doi.org/10.3389/fpsyt.2020.00001
North, C. S., Kawasaki, A., Spitznagel, E. L., & Hong, B. A. (2004). The course of PTSD, major depression, substance abuse, and somatization after a natural disaster. The Journal of nervous and mental disease, 192(12), 823–829. https://doi.org/10.1097/01.nmd.0000146911.52616.22
Norwood, A. E., Ursano, R. J., & Fullerton, C. S. (2000). Disaster psychiatry: principles and practice. The Psychiatric quarterly, 71(3), 207–226. https://doi.org/10.1023/a:1004678010161
Palinkas, L. A., & Wong, M. (2020). Global climate change and mental health. Current opinion in psychology, 32, 12–16. https://doi.org/10.1016/j.copsyc.2019.06.023
Thurston, A. M., Stöckl, H., & Ranganathan, M. (2021). Natural hazards, disasters and violence against women and girls: a global mixed-methods systematic review. BMJ global health, 6(4), e004377. https://doi.org/10.1136/bmjgh-2020-004377
Author and version info
June 21, 2023
Authors: Robin Cooper, MD and Lise Van Susteren, MD. Contribution from Afra Rahman, MS4
Editor: Colleen Rollins, PhD